



Abstrakt
Xronik anal çatın (AÇ) müalicəsində modifikasiya etdiyimiz üsulla posterolateral sfinkterotomiyanın (PLİS) effektivliyinin araşdırılması tədqiqatımızın əsas məqsədi olmuşdur. Material və metodlar: 2 il ərzində dorsal lokalizasiyalı xronik AÇ-a görə təklif etdiyimiz üsulla PLİS + fissurektomiya cərrahi əməliyyatı keçirmiş 19 xəstə müalicəmiz və nəzarətimiz altında olmuşdur. 18-62 il yaş aralığında olan xəstələrdən 11-i kişi, 8-i qadın olmuşdur. Bütün xəstələrdə PLİS (5 və ya 7 radəsində olmaqla) həyata keçirilmiş, sfinkterotomiya vizual nəzarət altında yalnız internal anal sfinkterin (İAS) distal 1/3 hissəsini əhatə etmişdir. Bu baxımdan oriyentirimiz dişli xətt (dentate line) olmuşdur. PLİS-in qənaətbəxş dozalanması üçün əməliyyat zamanı 33-34 mm diametrli obturatordan istifadə edilmişdir. 4 barmaq təftişi də praktik cəhətdən qənaətbəxş hesab edilmişdir. PLİS icrasından sonra dəri diliminin hərəkiliyini artırmaq məqsədilə dəri yara boyunca perianal istiqamətdə xarici anal sfinkterdən (EAS) iti surətdə 2-2,5 sm ölçüdə ayrılaraq mobilləşdirilmiş və fissurektomiya deffektinin bağlanması üçün flap hazır vəziyyətə gətirilmişdir. Güvənli fiksasiya üçün fissurektomiya deffektinin tikişlərinə İAS da hissəvi götürülmüşdür. Əməliyyatdan sonra spesifik ağırlaşmalar və residiv ehtimalı araşdırılmışdır. Modifikasiyalı PLİS + fissurektomiya əməliyyatı güvənli cərrahi nəzarətə sahib olmaqla bərabər, sfinkterotomiyanı əlavə kəsik aparmadan icra etməyə imkan verir; ağırlaşma və residiv riskinin cüzi olmasını nəzərə alaraq, xronik AÇ-ın cərrahi müalicəsində tətbiq edilə bilər.
Əsas mətn
INTRODUCTION
An anal fissure (AF) is a linear wound defect between the dentate line of the anоderm and the outer edge of the anus [1, 2, 3]. AF is a widespread proctological disease, occurring in all age groups with the same frequency for both sexes [4]. Although AF is mostly primary, it has not exact pathogenesis, but solid faecal excretion and hypertonicity of the IAS are considered to be the main factors of this pathology [5]. AF is manifested mainly with anal pain ± slight bright red bleeding with defecation [2]. If AF does not heal within 6 weeks, it can be recognized as chronic AF [4]. According to other authors’ mind, if the fissure is present for less than 8 weeks, it should be considered as acute AF. Chronic AF lasts longer and should be accompanied by one or more signs of chronicity (hypertrophied anal papilla at the proximal end of the fissure, sentinel tag at the distal end, and increased tone of IAS fibers along the fissure) [1, 2, 6, 7]. In most cases, AF is mostly located at posterior midline (90 %) and also it may be located at anterior midline (predominantly in women). In 3% of patients fissures can be located at posterior and anterior positions simultaneously. Fissures that located rather than the midline is considered to be atypical or secondary and needs more evaluation, because of possibility of association with serious diseases, like Crohn’s disease and immunodeficiency syndromes [2, 7]. The basing aim of the treatment of chronic AF is to relieve IAS spasm associated with a chronic fissure. Although medical treatment is effective in some cases, in vast majorities conservative measures fail. For such cases, surgery remains the gold standard of treatment for chronic АF [4]. Surgical methods for the treatment of chronic АF include anal dilatation, posterior midline internal sphincterotomy (PIS), lateral internal sphincterotomy (LIS), posterolateral sphincterotomy (PLIS), and fissurectomy with advancement flap repair [4]. Treatment has focused on alleviating hypertonicity of the sphincter. The most common surgical treatment is partial internal lateral sphincterotomy. In all types of surgical interventions, the main aim is to reduce sphincter hypertension. The most accepted type of surgical treatment is partial internal lateral sphincterotomy [4, 8]. A recent systematic review shows that patients treated with sphincterotomy have a cure rate of 95.13 %. At the same time, the positive results of surgery may be achieved at the cost of increased complications, especially persistent incontinence [9].
In the lateral position, internal anal sphincterotomy can be performed both by open and closed methods with almost the same effectiveness, being considered preferable than anal dilatation [10]. Posterior internal sphincterotomy (PIS) was proposed by Eisenhammer in 1951 as a midline incision along the fissure [11]. The aim of sphincterotomy during PIS was to cut the hypertonic part of the IAS muscle in order to reduce anal tone and facilitate fissure healing [12]. Although, in differ from LIS, the PIS can be performed through the same incision without creating a new wound [13], but prolonged healing time due to keyhole deformity and leakage of fecal material are considered as disadvantages of this procedure [1, 13]. However, if there is an intersphincteric fistula connected with the fissure, PIS can still be considered as an alternative treatment for chronic AF [13]. According to other authors’ mind, blindfold cutting of the internal sphincter during LIS leads to an increase of incontinence cases [14]. Some researchers noted that fissurectomy and sphincterotomy have the opposite effect [15, 16]. A sphincterotomy can be performed by a fissurectomy, in which a new surgical wound is created. So, by cutting the fibrotic fissure stable wound healing is provided [14]. According to several authors, LIS is recommended now as a standard procedure for the treatment of chronic AF [17, 18], because it is safe, effective and can be repeated [19, 20]. Several reliable studies come to conclusion that there is no significant difference between properly performed open and closed surgical sphincterotomy [7]. Excision of the IAS in LIS can be performed outside the fissure, in the right or left lateral positions under local, regional or general anesthesia, in the patient's lithotomy or prone jack-knife position, both by open or closed method [21]. Alawady M et all. comparing PLİS and LİS concluded that the time to complete healing was significantly shorter and pain score was significantly lower after PLIS than after LIS which can be due to more reduction in the resting anal pressure after PLIS. Continence disturbances occurred after PLIS less frequently than after LIS; however, no significant differences between the two techniques were noted [22].
Although various procedures are used in the treatment of AF, meta-analysis study found that for evaluation of the effectiveness of these different procedures more data are needed [23]. Early complications of sphincterotomy include bleeding, hematoma, bruising, perianal abscess, and fistula, but the most important complication is incontinence of different grades. Such cases are observed in up to 30% of patients, especially in patients with weaker, shorter sphincter muscles and in women who have suffered of mechanical damage of sphincter due to childbirth [21]. The aim of the research was to study the effectiveness and safety of fissurectomies completed by the posterolateral sphincterotomy (PLS) proposed by us in the surgical treatment of anal callous fissure in terms of symptomatic recovery, complications and relapses. Our main goal was to describe in detail the modified PLIS technique and its results in the surgical treatment of chronic AF. Therefore, we did not consider comparisons with other surgical treatments for chronic AF.
MATERIAL AND METHODS
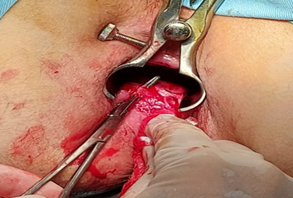
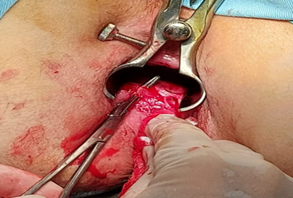
The patients with the diagnosis of primary chronic АF (located at 6 o’clock position) who underwent fissurectomy with modified PLIS were included in the study. The observations were carried out at the Educational Surgical Clinic of the Azerbaijan Medical University (Baku, Azerbaijan) during 2 years (2024-2025). Following the medical literature [2, 7], patients diagnosed with acute AF, tuberculosis, ulcerative colitis, secondary chronic fissure connected with Crohn's disease, and chronic AF, accompanied by hypotonicity of the anal sphincter were not included in this study. Besides, patients with associated proctological pathologies were also excluded from the study, because of their possible influence on the final results. The total number of patients was 19; 11 of them were men and 8 were women, the age range was 18-62 years (average age 38 years). The frequency rate according to gender and age was not statistically significant, our conclusion is generally consistent with the results of other studies [4]. All subjects were undergone fissurectomy + PLIS procedure at 5 or 7 o’clock positions by the same surgical team. This factor reduced to zero the possibility of subjective effects connected with different approaches to surgical results. During PLIS, only the distal 1/3 of the IAS was partially dissected, and a dentate line was taken as a marker. Visual control of PLIS allowed to perform optimal sphincterotomy and to achieve meticulous hemostasis (Figure 1). The results of our study are consistent with the facts we found in the medical literature on this issue [15, 16]. For evaluation of the satisfactoriness of PLIS, in the operation an anoscope obturator of 33-34 mm diameter was introduced into the anal canal. After the procedure, the free insertion of the obturator through the anal canal was considered as an indicator of the successful sphincterotomy. The 4-finger principle has been also applied as an equivalent to using an obturator. However, the use of an obturator was considered as more rational one. After performing of PLIS, for closing the fissurectomy defect and secure fixation of the skin flap the operations were continued as we proposed: initially, the skin flap was prepared so that it maintained its integrity and trophism. In order to increase the mobility of the skin flap, a 2-2.5 cm long section of skin was mobilized from EAS by sharp dissection in the perianal direction along the wound. After preparing the flap, when we started to tailor the medial part of the flap, slightly took the superficial fibers of the internal sphincter into the muco-cutaneous suture. It induced the fixation of the flap in the anal canal, supporting the mucosa to hold the sutures. So we found it useful for prevention of postoperative retraction. In order to minimize thermal tissue stress, it was considered more appropriate to use electrical devices as little as possible, to use cold (ice) throughout the operation, to achieve hemostasis by mechanical pressure and suturing. At the end of the procedure, perianal block by articaine+epinephrine 40 mg+5 mg/1ml injection (total 6-8 ml) and wound dressing with Metronidazole ointment were applied as auxiliary measures to reduce postoperative pain syndrome. The operations were performed under spinal (in most cases) or general anesthesia in the lithotomy position with bladder catheterization to prevent postoperative acute urinary retention and control diuresis. The indications for general anesthesia were patient's choice, including refusal of spinal anesthesia, impossibility of spinal anesthesia or anesthesia risks. Patients were followed 3 months, for assessing symptomatic recovery process and detecting early postoperative complications. Complications, such as bleeding, fever, incontinence, keyhole deformity, abscess and fistula forming; pain severity and recurrence rate were evaluated.
DISCUSSION
Anal manometry was performed in 17 patients 2 months after surgery, and only in 1 patient the resting pressure (RP) decreased to 38 mmHg. This case was assessed as 1st degree incontinence and was corrected conservatively. In other patients, postoperative RP ranged from 42 to 48 mmHg. Postoperative squeeze pressure (SP) was within the normal range in all patients. Information on early postoperative complications is presented in Table 1, and all complications that arose were resolved conservatively. Complications such as bleeding, keyhole deformity, abscess and fistula formation, disease recurrence, and the need for repeat surgery were not observed. Our results are generally consistent with statistical data found in the medical literature [4]. Medical parameters such as operation time, volume of blood loss, postoperative patient activation time, need for antibiotic administration, postoperative NSAID and narcotic analgesics use, and postoperative rehabilitation were investigated, and the results were found to be satisfactory (Table 2). The pain intensity measured by the VAS (the Visual Analogue Scale) was generally considered very weak, with less than 30 points. As part of our ongoing research, we plan to compare the proposed modified PLIS procedure with the standard LIS procedure.
CONCLUSION
Analysis of the results showed that visual control during fissureectomy with PLIS in all age groups, regardless of gender, allows for reliable dissection of the IAS of the required size without the need for additional incisions. Intraoperative use of a 33-34 mm diameter obturator is recommended to control the sphincterotomy volume. During the closure of the fissurectomy defect for secure fixation of the skin flap in the anal canal, taking superficial internal sphincter fibers into the muco-cutaneous sutures was beneficial in preventing the flap from immediate future displacement and also in avoiding of the keyhole deformity. The operation is comparable to alternative methods in terms of medical and technical aspects, financial costs, and medico-social rehabilitation indicators. Therefore, fissurectomy performed using PLIS can be considered an effective and safe procedure of choice for the surgical treatment of chronic AF, given the low risk of postoperative complications and recurrence.
Şəkillər
Açar sözlər
İstinadlar
1.Deari A. Ismaeil, Kamil Haydar, Ary Hama Saeed and Alaa Sabeeh Comparison between Open Lateral Sphincterotomy and Posterior Midline Sphincterotomy with Fissurectomy in Treatment of Chronic Anal Fissure/ Annals of Medical and Health Sciences Research | November-December 2019 | Vol 9 |; 640-643
2.Simmang CL, Papaconstantinou HT, Jr. Fissure-in-ano PJH. In Shackelford’s Surgery of the Alimentary Tract Elsevier Saunders, USA. 2013 pp. 1907-1310.
3.Leong AP. Pharmacological treatment of anal fissure-A future role in primary care. // Singapore Medical Journal. 2003;44:136-140
4.Mohammed Alawady, Sameh Hany, Emile Mahmoud, Abdelnaby Hosam, Elbanna Mohamed Farid/ Posterolateral versus lateral internal anal sphincterotomy in the treatment of chronic anal fissure: a randomized controlled trial. // International Journal of Colorectal Disease. Volume 33, pages 1461–1467 (2018)
5.Ayantunde AA, Debrah SA. Current concepts in anal fissures. // World Journal of Surgery. 2006; 30. 2246-2260
6.Golfam F, Golfam P, Khalaj A, Mortaz SS. The effect of topical nifedipine in the treatment of chronic anal fissure. // Acta Medica Iranica. 2010: 295-299.
7.Stewart Sr DB, Gaertner W, Glasgow S, Migaly J, Feingold D, Steele SR. Clinical practice guideline for the management of anal fissures. Diseases of the Colon & Rectum. 2017;60:7-14.
8.Shao WJ, Li GC, Zhang ZK (2009). Systematic review and meta-analysis of randomized controlled trials comparing botulinum toxin injection with lateral internal sphincterotomy for chronic anal fissure. // Int J Colorectal Dis 24: 995–100
9.P. A. Boland, M. E. Kelly, N. E. Donlon, J. C., Bolger, J. O., Larkin, B. J. Mehigan, et al. “Management options for chronic anal fissure: a systematic review of randomised controlled trials” // Int. J. Colorectal Dis., vol. 35, no. 10, pp. 1807-1815, 2020.
10.Nelson RL. Meta-analysis of operative techniques for fissure-in-ano. // Diseases of The Colon & Rectum. 1999; 42: 1424-1428
11.Eisenhammer S. The evaluation of the internal anal sphincterotomy operation with special reference to anal fissure. // Surgery, Gynecology & Obstetrics. 1959; 109: 583.
12.Eisenhammer S. The surgical correction of chronic internal anal (sphincteric) contracture. // South African Medical Journal. 1951; 25: 486-489.
13.Memon AS, Siddiqui FG, Hamad A. Fissurectomy with posterior midline sphincterotomy for management of chronic anal fissure. // J Coll Physicians Surg Pak. 2010; 20: 229-231
14.Abdul Sattar Memon, Faisal Ghani Siddiqui and Adeel Hamad Fissurectomy with Posterior Midline Sphincterotomy for Management of Chronic Anal Fissur. // Journal of the College of Physicians and Surgeons Pakistan 2010, Vol. 20 (4): 229-231
15.Lambe GF, Driver CP, Morton S, Turnock RR. Fissurectomy as a treatment for anal fissures in children. // Ann R Coll Surg Engl. 2000; 82:254-7. 11.
16.Mousavi SR, Sharifi M, Mehdikhah Z. A comparison between the results of fissurectomy and lateral internal sphincterotomy in the surgical management of chronic anal fissure. // J Gastrointest Surg 2009; 13:1279-82. Epub 2009 May 5
17.Nahas SC, Sobrado CJ, Araujo SE, Aisaka AA, Habr-Gama A, Pinotti HW. Chronic anal fissure: results of the surgical treatment of 220 patients. // Revista do Hospital das Clínicas. 1997;52:246-249
18.Acar T, Acar N, Gungor F, Kamer E, Gungor H, Candan MS, Bag H, Tarcan E, Dilek ON, Haciyanli M. Treatment of chronic anal fissure: is open lateral internal sphincterotomy (LIS) a safe and adequate option? // Asian J Surg. 2019; 42: 628–633.
19.Nessar G, Topbas M. Lateral internal partial sphincterotomy technique for chronic anal fissure. // Indian Journal of Surgery. 2017; 79: 185-187.
20.Sarkar S, Kapur N. Lateral internal sphincterotomy under local and spinal anaesthesia for chronic anal fissure: A randomized control trial. // Hellenic Journal of Surgery. 2016; 88: 398-401
21.Lunniss P. The anus and anal canal. In Williams N, O’Connell PR, McCaskie A. Bailey & Love’s Short Practice of Surgery: The Collector’s Edition. CRC Press; 2018;1351- 1353
22.Mohammed Aawady, Sameh Hany Emile, Mahmoud Abdelnaby, Hosam Elbanna, Mohamed Farid. Posterolateral versus lateral internal anal sphincterotomy in the treatment of chronic anal fissure: a randomized controlled trial. Int J Colorectal Dis. 2018 Oct;33(10):1461-1467.
23.Nelson RL, Chattopadhyay A, Brooks W, Platt I, Paavana T, Earl S. Operative procedures for fissure in ano. Cochrane Database of Systematic Reviews. 2010.
Məqalə barədə təfərrüatlar:
Nəşr tarixçəsi
Dərc edilib: 07.Apr.2026
Müəllif hüququ
© 2022-2025. Azərbaycan Tibb Universitetinin nəşri. Jurnalın elektron versiyası "Uptodate in Medicine" tibb nəşriyyatı tərəfindən dərc olunur. Bütün hüquqlar qorunur.Əlaqəli məqalələr
Baxılıb: 919